

In the earliest and darkest days of the pandemic last year, health experts were plagued by a lack of coronavirus testing, long wait times for results and an incomplete picture of what was driving outbreaks.
Now, more than a year and a half later, many public health professionals are confronting the same issues.
The delta variant is fueling a devastating new surge of infections, but experts say declines in testing and a lack of granular data about hospitalizations make it difficult to know just how much the virus is circulating in communities — and who remains most vulnerable.
That makes it harder to control new outbreaks, including those in schools as students return. It also hampers scientists’ ability to catch other, potentially more worrisome strains that may emerge.
“Without adequate data, policymakers are just swinging in the dark,” said Dr. Jeffrey Klausner, a clinical professor of population and public health sciences at the University of Southern California. “What you get is a discordant response and somewhat chaotic policies that frequently change, and people are left worse off.”
Aug. 18, 202102:18
Most experts agree that official case numbers probably undercount the true number of Covid infections in the country. Those falling through the cracks are likely to be asymptomatic cases and people who experience only minor symptoms, said Dr. Benjamin Lee, a pediatric infectious disease physician at the University of Vermont.
What that means is that communities are left with a murky picture of where and how the virus is spreading, at least until hospitalization rates, which lag behind infections, start to creep up. That is particularly true with potential breakthrough infections in fully vaccinated people, Lee said.
“There’s sort of the assumption that if I’m vaccinated, I’m protected, so very mild symptoms that may have prompted testing over the winter just aren’t being picked up right now,” he said.
And because the vast majority of breakthrough cases are mild or asymptomatic, people with breakthrough infections may not even know to get tested and could thus transmit the virus unknowingly. Evidence that vaccinated people could readily spread the virus was what caused the Centers for Disease Control and Prevention to declare in internal documents last month that “the war has changed” with the delta variant.
But even that was based on limited data.
“Probably our biggest deficit now is knowing how many of those mild and asymptomatic cases are contributing to ongoing transmission that could subsequently lead to more hospitalizations,” Lee said.
Criticism of the overall lack of data has gained steam in recent weeks. Dr. Scott Gottlieb, a former commissioner of the Food and Drug Administration, tweeted Sunday that the U.S. still has major gaps in its understanding of the current wave of infections.
“In the U.S. we have no firm idea how many kids have already been infected with COVID,” Gottlieb wrote. “We have no idea if hospitalizations in south are tip of a huge iceberg of dire infection — or a sign that COVID has become more pathogenic in children. The CDC should gather this data. It isn’t.”
Emily Oster, an economics professor at Brown University, echoed Gottlieb’s sentiment, arguing that the U.S. needs a “data force” that could be mobilized to gather information about, among other things, breakthrough infections in fully vaccinated people and Covid cases in children.
“The fact is that 18 months into the pandemic, we are still not in the position we should be, in terms of our ability to move quickly to collect and analyze data that is needed for public health decisions,” Oster wrote Monday in her online newsletter.
That may change soon. The CDC announced the creation of a disease forecasting center Wednesday to assess emerging health threats and help guide public health decisions by governments, businesses and communities.
The initiative will probably focus much-needed national attention on addressing infectious disease risks. Klausner, who previously worked for more than a decade at the San Francisco Public Health Department, points to the country’s fractured public health system, which leaves decisions about what to monitor and report up to counties and states, as a major reason for the lack of cohesive data. But declines in coronavirus testing nationwide also play a role.
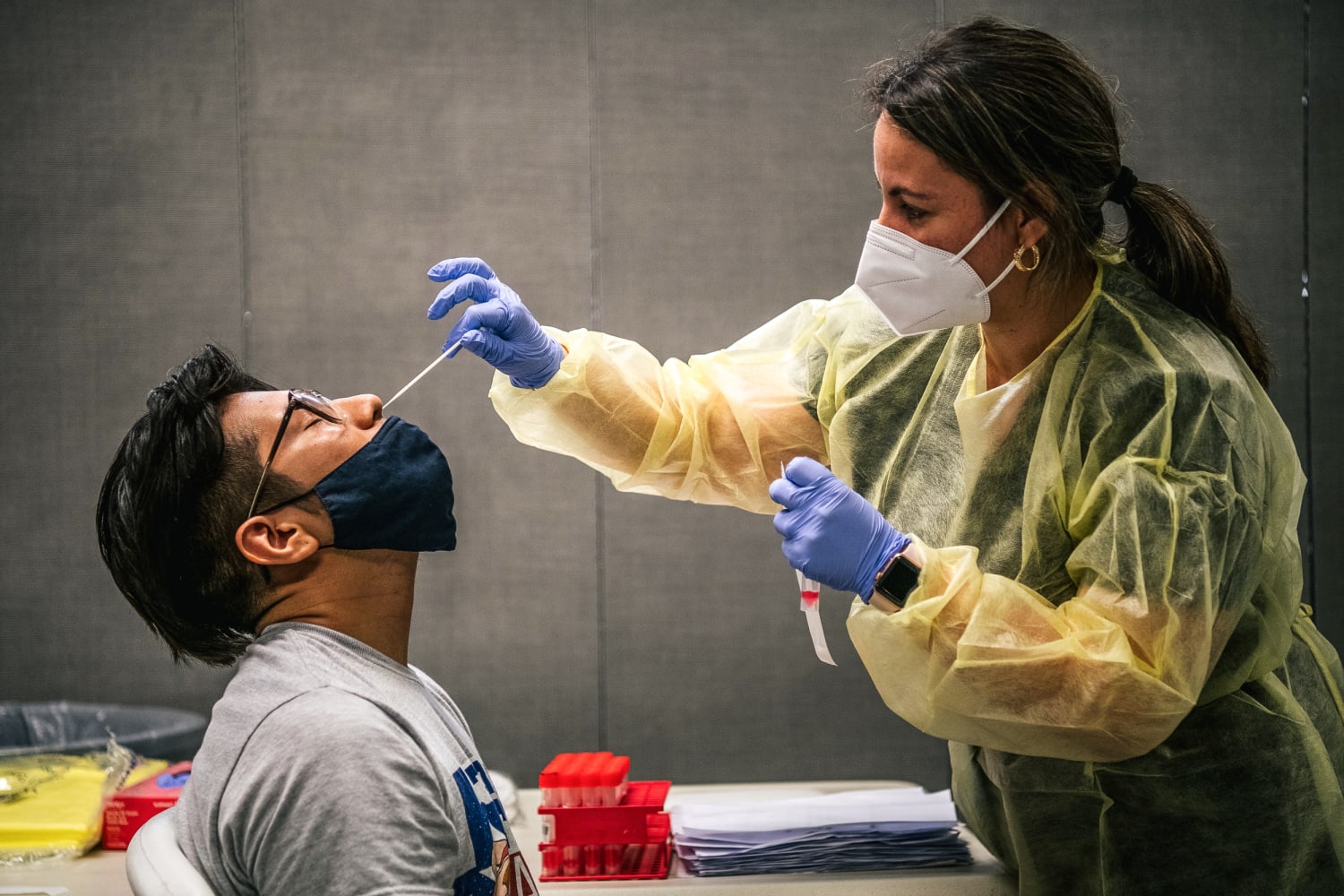
Testing slowed significantly across the country over the spring and summer, largely in response to vaccinations that helped flatten case counts and offered a brief respite from widespread community transmission. The number of tests administered daily in the U.S. peaked in January, according to data from Johns Hopkins University, and it fell precipitously over the following months.
Without more detailed information about who is getting infected, it’s difficult for public health officials to craft specific policies to protect those at risk, said Dr. William Raszka, a pediatric infectious disease specialist at the University of Vermont. The problem is all the more urgent as millions of children, including young children who aren’t yet eligible for the Covid-19 vaccines, are returning to classrooms for the new school year.
“The whole start of this school year has been anxiety-provoking for me,” Raszka said. “Last year was very straightforward. The governor had emergency powers and said everyone has to mask. That was easy and straightforward. Now it’s ridiculously confusing.”
More widespread testing at schools and other places could help scientists establish baselines that would enable them to better characterize the virus and compare case rates and severity between age groups and other demographics, Raszka said. As it stands now, it’s not well understood whether rising cases and hospitalizations in young children are because children are more susceptible to the delta variant or simply because young children make up a big part of the unvaccinated population in areas where the virus is circulating widely.
Even in a state like Vermont, where about 80 percent of the eligible adult population has been at least partly vaccinated, testing has become an issue, Raszka said.
“In some areas, the testing sites shut down because nobody was using them and it was expensive to keep them open,” he said. “That shrank our capacity to do testing once things ramped up because of delta.”
As a result, wait times for test results are also up in places where the delta variant is already straining public health resources.
Another part of the problem is that people seem less likely to get tested now than in earlier stages of the pandemic, particularly if they have only mild symptoms, said Rita Burke, an assistant professor of clinical preventive medicine at the University of Southern California.
It leaves open the question of how to encourage people to start seeking out tests again.
“People are definitely more knowledgeable now about the symptoms and how important it is to self-isolate,” Burke said. “We know that not everyone who is positive gets tested.”
A more comprehensive understanding of the situation on the ground could guide officials in how to balance the needs of their communities.
“It becomes a staffing and resource issue,” Burke said. “We decreased capacity for testing because the focus shifted to vaccinations, and we need staff for that.”
Scientists are therefore left with a less-than-perfect understanding of how the virus is spreading and what is driving community transmission.
In addition to helping public health departments track the spread of the virus, regular testing can help scientists spot changes in the pathogen. If researchers don’t have a firm grasp on what virus strains are circulating in the country, new variants may not be detected until it’s too late, Lee said.
“We’ll be vulnerable to the same types of challenges if, God forbid, another variant comes along that is more infectious than delta,” he said, “or is more successfully able to evade vaccine protections.”
For now, one of the most reliable indicators in a community is its hospitalization rate. But hospitalizations can lag by up to two weeks behind infections, so they may offer only snapshots of the virus’s prevalence. And hospitalization data don’t often drill down into specifics of new patients’ vaccination statuses, occupations or household situations or whether they were previously infected — all valuable information for crafting public health policy, Raszka said.
Still, once hospitals start to fill up, it’s typically an unambiguous indication that an outbreak may be spiraling out of control.
“We know that a lot of our hospitals are in trouble across the Southeast: Case volumes are up, and they are overloaded,” said Dr. Marybeth Sexton, an assistant professor at the Emory University School of Medicine. “Regardless of the cause, we know that’s happening on the ground.”
Sexton said it makes sense in this phase of the pandemic to devote resources that were previously earmarked for testing toward vaccination efforts.
“As important as testing can be in the moment for getting people in treatment or doing contact tracing, testing is not going to end the pandemic,” she said. “Vaccination will do that.”
Source: | This article originally belongs to Nbcnews.com







